Here I am, in it, curled as you are, as all are who breathe.
I found myself here, not by my choice but by that of something other. So, I’m here wondering how you interpret the mystery of it —not its biology, but the phenomenology of it, the cloud of meanings of its textures and structures, the before, now, and after of it, the all-and-what’s-next of it curled as we are in this womb of now, waiting, anticipating new birth in a next moment, waiting to be thrust beyond by the pulsations of past moments.
Jim Culleny, 6/21/26
Enjoying the content on 3QD? Help keep us going bydonating now.
My cat died of pancreatic adenocarcinoma a few weeks ago. In March she had an annual check up and was deemed to be in good health for 13, although a bit overweight. We noticed that she was walking a little funny sometimes, so the vet suggested we think about arthritis medication. Then one day in May, just before our appointment to start meds for her suspected arthritis, she went into hiding. A more in-depth vet appointment discovered that her changed gait wasn’t from her joints, but from a huge abdominal mass. It took some tests to find out what it was, then came the dreaded decision-making about what to do about it. Apparently cats can live for months with the condition but often with a very dismal quality of life.
BURYING DIFFICULT PERSONALITIES
She was an ornery cat despite living a life of safety and comfort. I have a certain respect for the fact that she’d snap if you pet her one too many times or in a way that she didn’t want today. She was my work companion, often snuggled in beside me during online school sessions or marking marathons, but there was more than one time during a meeting that she suddenly attacked my arm if I gestured too widely, and I had to feign nonchalance as I shook her off me just outside of camera range. And she was always a bit dirty. As soft as she appeared, her fur acted like velcro, tracking litter throughout the house. Despite regular brushing, wherever she curled up, she left behind the expected layer of hair, but also bits of gravel and maybe some sticks and leaves. Of course she loved to sleep in my bed under the covers. (And who could say no to a tiny mew beckoning to be let in?) I feel asleep to her purrs, but I’d often be rudely awakened by a few sharp bats to the head if I moved around too much. She either couldn’t learn or didn’t care that disciplining me would cost her bed-privileges for the rest of the night.
I had her undeserved adoration from the day we took her and her sister home. For a good year after we started letting her out, if I’d go for a bike ride, I could turn to see her running down the street after me (a very safe, quiet street). While I admired her feistiness, I often loved her in spite of her personality. And I wonder how much I held her in a special place of honour because she chose me, and if that “counts” as love.
It’s complicated burying loved ones with whom we have a complex relationship.
On top of the grief, I have some guilt. I haven’t just accepted her death; I was kind of looking forward to it. It sounds horrible and uncaring, but there it is. Maybe it’s from my Jungian dominant function being task-oriented (aka thinking-type) so I might see what needs to be done more than the people or animals in front of me. It’s a sense of “What’s next on the list?” like gleefully anticipating reading a good book at home once we can make an exit from a party. A future-focus can keep us engaged and productive, but can also keep from actually existing in the present. That’s certainly one way to look at it, but I don’t think that’s the whole story. Read more »
You can’t be the leader of a small island nation in Southeast Asia without a sharp focus on China. While Singapore as we know it was founded by the British and the modern Republic of Singapore by and large adopted British institutions – it no longer relies on its colonial parent for either security or trade.
Instead, Singapore – like so many countries in Southeast Asia – finds itself preoccupied with the United States, its largest security partner – and China, its largest trade partner with particular respect to exports. Singapore built a thriving economy based on its unique position of culturally and linguistically straddling East and West. Its people understand not just the words, but the ideas and minds of both Orient and Occident.
Singapore’s long-governing, founding Prime Minister, Lee Kuan Yew was an ardent anti-communist who in 1965 said things like:
I cannot in all honesty say that communism is a diabolical evil, because I can imagine certain human societies where it was a great relief to have the communists displace a ruling power. That is another of the very difficult problems we face in this country. To some 600 million Chinese, that philosophy was the answer and is the answer to a decadent, a corrupt and an evil society which has become evil because men have lost their self-respect and lost their values.
Yet, later in his career he became a consultant to Deng Xiaoping, helping China plan reforms that would transform it from its former truly communist self to the more capitalist, albeit authoritarian state we know today. To Lee, moving China toward capitalism and participation in the world economy was a net positive. China being part of a cooperative global order was the attainable win that would make the world safer. Read more »
The guillotine at Hoa Lo Prison in Hanoi. All photos taken by Daniel Gauss.
When I went to Hanoi for the first time, I began a travel ritual I now follow in every city I visit.
I had grown up reading about the Vietnam War, mostly from our perspective, but still grim and unflinching, full of failed policy and the atrocities our military carried out. It was not just the insane level of the violence but its cruel senselessness that affected me, that so much suffering and death had been meted out gratuitously and malevolently by military and political leaders who knew we could not win. We kept killing innocent people and sacrificing our own troops, long after it was clear we should have stopped.
Because it was my country that inflicted the egregious pain and my own compatriots who were harmed by the war, it unsettled me deeply and tore apart the benevolent image of my country I had been taught. I knew that going to Hanoi would be more emotional than any trip I had taken before.
I felt I couldn’t just show up in Hanoi, I needed to go somewhere meaningful on my first day and offer a type of silent prayer. I now find a meaningful place in every city I visit to offer a prayer for those who have suffered. Read more »
As a species of Jew, the child of a self-declared “violent atheist” Jew and a gentile mother, I’ve found some use in the Jew vs. Zionist distinction. Long before October 7th and the genocide in Gaza, I’ve found it hard to extricate the history of Israel from the erasure of the Palestinian people. Please look around for a clip of Rabin revealing what Ben Gurion told him about Palestinian villages in the late forties if you doubt that conclusion.The Jew/Zionist distinction has allowed me to remain proud of my Jewish heritage while distancing myself from Israel.
But rage against “Zionists” has recently begun to seem broader than disdain for Israel.While it was comforting that Khymani James, a student leader of the pro-Palestinian movement at Columbia University thought only Zionists (not Jews) deserve to die and that we should be “grateful” that he was not “just going out and murdering Zionists,” I wondered why he was threatening to kill people and how killing supporters of Israel in New York would help Palestinians in Gaza.
But the Jew/Zionist distinction really lost ground with me after Jared Moskowitz, a democratic congressman from Florida, received death threats over the phone proclaiming the need to “kill every single fucking Zionist scumbag” because “the US. Government needs to kill Jews.”And then, of course, there has been Tucker Carlson’s sudden opposition to Trump in part because of his “globalist” sympathy with Israel and Jews. These haters clearly hold no distinction between Zionists and Jews. And none of them (clearly racist) show any concern for Palestinians.
Of course, I was worried and saddened to hear all this as a Jew myself and a person who wants, as Rodney King so plaintively put it decades ago, for people to “just get long.” But it also revealed a problem with what had once seemed like a useful term. Read more »
From the Dept. of Shower Thoughts (literally, this morning): I keep seeing, especially as advice for young people, that the skill needed to thrive in our AI dominated, rapidly transforming future is going to be the ability to continually learn new things and skills and being “adaptable”. Okay, I guess in some ways it is a good thing to learn new things and new skills (even I do so from time to time, remember my choir singing from a couple of years ago? ). But newness also brings stress and anxiety. Most of you will remember your first day at some new school and the dread and anxiety of that experience, simply caused by everything being new. And every new thing brings that to some degree or other, I think. We can deal with this comfortably if the changes come at a certain pace, but beyond that, we may all experience what I have been experiencing over the last year in trying to stay on top of what the frontier AI models are capable of and how I can use them: severe stress and CONSTANT learning of an ever-changing subject. How I do some routine things this month is not going to be the same as I do those things next month. This is becoming too much for me already. So, is re-living the first day in a new school every month or every week what all our futures are going to look like? If so, I will need all the Xanax I can get my hands on!
P.S. Related thought: The newest form of polarization in society is people who emphasize the ways in which AI is different from human brains vs. the people who emphasize how they are similar. They are, of course, both. So you can find plenty of evidence for whichever side you support.
P.P.S. Please give some feedback on whether my sharing these barely formed thoughts here on 3QD is good or just a waste of your time!
***
Enjoying the content on 3QD? Help keep us going by donating now.
This is a lightly edited transcript of an online video conversation. You can get more information about Ravi Shavi’s new album Wild Rock Dove here. Instagram link here.
Abbas and Rafay talking online
Abbas: I’m happy to have Rafay Rashid with me today and now I’m just going to read the bio he sent me: “Rafay was born in Islamabad, Pakistan, and grew up in New York and Rhode Island. He makes experimental pop and no-wave songs under the moniker Ravi Shavi that are confessional, ecstatic, and confrontational. His writing emerged as a response to growing up a Muslim kid in the neoliberal hellscape of post-9/11 America. Ravi Shavi became a persona and vehicle for both radical healing and anarchic humor as he crafted a niche amid the noise and freak-folk music scenes of Providence, Rhode Island, in the late aughts. Since then, he has cut his teeth touring independently throughout the past decade, opening for such acts as Charles Bradley, Of Montreal, Man Man, Budos Band, Los Lobos, and The Black Lips. Ravi Shavi will be performing with Spoon on June 19, 2026, in Providence, Rhode Island. He has a new album coming out, which is what we are here to talk about. It is called Wild Rock Dove.”
So, Rafay, thanks for coming. It’s good to see you.
Rafay: The biography sounds so loaded coming out of your mouth.
Abbas: People compare my personality to that of a shotgun. I can be loaded; I can also be locked.
Rafay: I was picturing the Ken Burns effect, with photographs from my life. I had never pictured that while reading the bio before, so thank you for that. Thanks for having me.
Abbas: Sure thing. Just to let everybody else know, I really like Rafay’s music. Full disclosure: Rafay is a friend, and in some distant way, through marriage, we are also related. No blood relation, as far as I know.
I have only met Rafay a few times, but it has always been real, and we have always had interesting conversations. And, as I already said, I love his music. I heard one of your songs today, Rafay, not completely deliberately but because several of your songs are part of my exercise playlist. As I was doing a little workout, your voice came on.
A song from one of Rafay’s older albums
You have done so many things. You got a master’s in… tell me about that. In what?
Rafay: In mental health counseling, or, more colloquially, therapy. It was something I had never really seriously considered for myself until my own process of getting sober. I don’t know why they always call it a journey, getting sober, but I got sober in 2020. Then the pandemic happened, gigs started slowing down, and the work I was doing on art exhibitions had ended and dried up. So I thought, well, I had a good time in rehab. Maybe I could run some groups. I always liked socializing with people and getting the conversation going. Read more »
London Falling opens in late 2019 when nineteen-year-old Zac Brettler steps onto the balcony of a luxury apartment in London and jumps. The building sits directly across from Britain’s intelligence service MI6, which is how the Metropolitan Police came to have the surveillance footage of what happened.
The police suggested suicide. But Zac’s parents did not believe them. They do however acknowledge that there were some red flags about their son’s recent behavior. In the previous year, they tell the police, Zac had been spending quite a lot of time in the company of two older men. One of them, Verinder Sharma fifty-five, was allowing Zac to practically live with him in that luxury apartment across the river from MI6. The cameras showed that Sharma, also known as “Indian Dave,” was in the apartment when Zac jumped. But so was another older man named Akbar Shamji.
When Zac’s parents questioned their son about his relationship with these men, the teenager explained that they were successful businessmen and were mentoring him. Sounds strange and yet having a son about Zac’s age, who also studies business in university, I can imagine a similar scenario. Like Zac, my son is personable and enthusiastic to learn how businesses are run, so I can see him shadowing a friend’s father at work or playing golf with one of them. He does things like that already. But still, Zac’s parents were concerned about it—mainly because it was so much.
And anyway, what kind of businesses were these men running? Read more »
A couple of weeks ago I saw an item in Lit Hub Daily, about how June 4th would be the 86th anniversary of the publication of The Heart is a Lonely Hunter, Carson McCullers’ debut novel. This item brought back many wonderful memories — of the novel, of the time in my life when I read it, of the movie made of it, and of an uncanny coincidence.
But the novel itself was an outlier. It did not fit any of the accepted and expected categories of mainstream fiction. It was neither a love story nor a bildungsroman, it did not have characters whom readers could recognize as like themselves, it did not have a happy ending, and it did not have a single strong narrative line. Instead, it followed a striking group of oddballs and misfits, the inhabitants of a small Southern city who individually take their hopes and fears to another oddball and misfit.
The other oddball and misfit to whom all hopes and fears are taken is named John Singer. Singer is a deaf-mute, who cares for, in both senses, another deaf-mute, a man with mental illness named Antonapoulos. Eventually Antonapoulos is committed to an asylum, and Singer must move to another small town in Georgia to be near him. He takes a room in the home of Mick Kelly, a teenage girl whose father has been injured in a work accident and is no longer employed; the family is poor and has to take in boarders. Mick is full of all the things teenagers are full of: hopes, dreams, longing, desires, anxieties, fears, and everything else. Read more »
The Republican Party has forever faced a serious statistical obstacle: There are always more Democrats. Never once since the GOP was founded in 1854 have there been more registered Republicans than Democrats in the United States. Democrats are always more numerous. So how can Republicans win?
You have to shoot every angle. You have to get lucky. And when sharp angles and dumb luck run out, you eventually you have to bend the rules.
The party’s rise, specifically the election of Abraham Lincoln as president with just under 40% of the popular vote in 1860, precipitated cession Democrats’ withdrawal from U.S. government and the start of the Civil War. During the war, the remaining United States was effectively under one-party Republican rule. Despite this, Northern Democrats remained a force in U.S. politics. When Lincoln ran for re-election in 1864, with only Union states participating, Democrat George McClellan still pulled nearly 45% of the popular vote.
Lincoln had hoped to build Republican support in the South after the war through a coalition of newly freed Blacks and Southern Whites who had opposed cession. However, his assassination placed Southern Democrat Andrew Johnson in the White House, easing former Confederates’ path to regaining U.S. citizenship and voting rights. Former Confederates then waged terroristic campaigns against new Black voters and White sympathizers to regain control of Southern governments. By the time political Reconstruction ended in the 1877, White Democrats in all Southern states, including formerly loyal slave states Maryland and Tennessee, were using the Democratic Party to establish white supremacist apartheid throughout the region.
Republicans were banished to permanent minority party status in the South, and aside from occasional hiccups, the region would remain under one-party Democratic rule for over a century. Read more »
Here’s your chance to say what you want to the large number of highly educated readers that make up 3QD’s international audience. Several of our regular columnists have had to cut back or even completely quit their columns for 3QD because of other personal and professional commitments and so we are looking for a few new voices. We do not pay, but it is a good chance to draw attention to subjects you are interested in, and to get feedback from us and from our readers.
We would certainly love for our pool of writers to reflect the diversity of our readers in every way, including gender, age, ethnicity, race, sexual orientation, etc., and we encourage people of all kinds to apply. And we like unusual voices and varied viewpoints. So please send us something. What have you got to lose? Click on “Read more »” below…
When I was a physics graduate student at Arizona State, one of my fellow grad students had a roommate who, after obtaining an undergraduate business degree, got a job as an office assistant for an economics professor. The roommate (remember, not a grad student) was earning like a young professional, not a wizard’s apprentice. “You know what he’s doing this week?” the grad student told us during a typical lunchtime rant. “He’s downloading files one by one from a dot-gov website and copying them into spreadsheets. A week of work, for what I could write as a five-minute script! And he’s getting $60,000 a year for this!”
Whether or not $60,000 sounds like a lot of money depends on one’s position. My whole life, I have seen claims the median physics B.S. graduate makes that much, but I personally didn’t make $60,000 until my third year as an assistant professor—and, even then, only after getting another job and negotiating a raise.
Science Nonfiction: Behind the Scenes in University Research, the new memoir from Dr. Darren Lipomi, chair of the Department of Chemical and Sustainability Engineering at the University of Rochester, addresses such issues bluntly—until it doesn’t. “There is a fair case to be made that the financial burden of research is borne not by the taxpayer,” Lipomi writes, “but by the ‘forever trainee’—the twenty-two-year-old PhD student who becomes a postdoctoral scholar at twenty-nine, and an untenured research scientist at thirty-four.” But now in his mid-forties, having more or less figured the system out, Lipomi is doing better than fine, and his memoir charts an uneasy path between celebration and critique. Read more »
About ten years ago, I received an invitation to coffee from a fellow I hadn’t seen in a while. At the time, Rolf Kuhn was teaching English at a middle school in the nearby town of Baden; our acquaintance was the result of our frequenting the same English-language bookstore—Pile of Books, still run in those days by our common friend Dani Nufer—in Zurich, where we both lived. The gap in our regular contact had been due to a caesura in my personal life, which had occasioned a lengthy stay abroad, and did not reflect any deterioration of our friendship.
We met, at Rolf’s suggestion, at a place called Chez Marion, across from Zurich’s central library and just up the slope from Rudolf Brun Bridge over the Limmat. Chez Marion, which has since ceded its location to a schnitzel restaurant, was a French bistro in the evenings and an old-fashioned Zurich café by day, with curtains in the windows and frilly paper round the stems of tea glasses. Just the place for a chat with a Swiss teacher approaching retirement, I thought.
And indeed, the coming change in Rolf’s employment status soon came up, and I asked him what he was planning on doing with his free time.
“I’m going to break into the testing center at a Big Pharma company,” he responded without hesitation, “and free all the lab animals.”
Rolf Kuhn
This wasn’t the answer I had been expecting to hear, from a white-haired Swiss burgher in such well-mannered surroundings. But I really shouldn’t have been surprised. After all, in the late 1990s and into the early years of the new millennium, while working at the middle school and in accordance with Switzerland’s Milizprinzip, which envisions politics as a part-time job to be performed not by professional legislators but by specialists in a variety of trades, Rolf had served in Zurich’s city parliament, or Gemeinderat, where he represented the Socialist Party and spoke up frequently on issues of social justice and environmental protection. Furthermore, one of the occasions on which he and I had first met, years earlier, at Dani’s bookshop was the time I performed an acoustic set there with The NewMen, a country-punk outfit for which I once provided lyrics and vocals—and Rolf’s enthusiasm for our rough-and-ready show that evening had been wholehearted. Finally, if only symbolically, with his walrus moustache and rugged good looks Rolf could have passed as the long-lost brother of Georges Brassens, France’s celebrated anarchiste punk troubadour, whose most notorious ballad, “Le gorille,” features an animal escaping from confinement to wreak havoc among the hypocritical patrons of a zoo… Read more »
[I]t was the first solemn declaration by a nation of the only legitimate foundation of civil government. It was the corner stone of a new fabric, destined to cover the surface of the globe. It demolished at a stroke the lawfulness of all governments founded upon conquest. It swept away all the rubbish of accumulated centuries of servitude. It announced in practical form to the world the transcendent truth of the unalienable sovereignty of the people. It proved that the social compact was no figment of the imagination; but a real, solid, and sacred bond of the social union. —Secretary of State John Quincy Adams, July 4, 1821.
John Peter Zenger printing press, Federal Hall National Memorial, New York, NY.
On some past Fourth of July, their store closed for the holiday, my parents packed up a pair of children, hats and sunscreen, coolers filled with salami and roast beef sandwiches, sliced red peppers and cucumbers, and bottles of soda “to wash things down.” Plus a pair of Rolleiflex cameras and rolls upon rolls of Agfa film (with 12 shots to the roll, you needed a lot of rolls). There were also maps (of the paper kind) and towels (of the cloth kind), sunglasses (prescription and flip-up), and packets of Sun-Maid Raisins and Planters Peanuts, just in case we got lost and had to live off the land. Important to be prepared.
North on the Taconic Parkway we went, through Westchester, through Putnam to Dutchess—destination some town or hamlet that would be having a Fourth of July celebration. I rooted for proximity to the Old Rhinebeck Aerodrome, where, along with patriotism on display, there were also biplanes, but, on this occasion, I don’t recall the merging of the secular and religious. The town for which they chose to turn off the road did not have a Sopwith Camel, but it did have a Fourth of July celebration and parade.
Signs, flags, buntings, displays. Food stands. High school marching band, leading a group of what were likely local worthies. Middle-aged WW-II vets in their (slightly tight) uniforms, their families waving at them as they went past. A fire truck. Vintage cars, and particularly the big open ones that carried the WW-I vets—everyone clapped and waved at them. How could you not?
Somewhere, at some point, the parade ended in a town square, with people merging in front of a set of stands and a podium, and, from there, a local worthy (a Mayor, perhaps even a Congressman) got up from a chair and delivered a Fourth of July Speech. Perhaps it wasn’t quite up to John Quincy Adams’s offering, but it was the kind of speech that recalled a great moment of our past and urged us to reaffirm our commitment to the ideals expressed that day. Read more »
Tycho Brahe was a significant figure in my family. Why? Because my father’s parents were from Denmark, and Tycho Brahe was Danish. Danes were thus important in the Benzon household, as was Danish pastry (wienerbrød, Vienna bread), the real stuff with cardamom seeds, not the fluff you get in diners. And then there is rabarbergrød, a cloudy translucent rhubarb pudding laced with slithers of almonds. Not to mention Danish layer cake, five thin cookie-like layers alternating with custard and currant jelly topped with a lemon-juice & powdered sugar icing, once a year on my father’s birthday. But I digress.
We were told about Leif Erikson, who made landfall in the Americas half a millennium before the Italian. About King Christian X, known for his defiance of Hitler, which – wouldn’t you know? – became embroidered with legend. But most important of all, Victor Borge, an important comedian in mid-century America known for his dry wit and use of music as a comedic medium, which called forth his considerable skill as a concert pianist.
Whoops! I digress.
This essay isn’t about desserts, kings, or even comedians. It’s about a living intellectual, the economist Tyler Cowen. I won’t bother with boilerplate basics, you can find that in Wikipedia. As for his similarity with that long-deceased 16th century Danish astronomer, Tycho Brahe, we need to have some appreciation for what Cowen has done before stacking him up against the dead Dane.
First up, Cowen’s blog. Then we blitz through a list of 59 people he’s interviewed (out of 279 so far), then on to philanthropy, after which we slow way down to look at his current monograph, The Marginal Revolution: Rise and Decline, and the Pending AI Revolution. When we’ve gone through that we’ll understand the comparison with Tycho Brahe.Read more »
Last monsoon, I was watching a group of students in a classroom in Coimbatore settle into a difficult conversation. Two students had reached an impasse over something that genuinely mattered — a disagreement about a community project that had moved from practical to personal without anyone quite deciding it should. The room had that particular quality of charged suspension when everyone is watching to see what the adults will do.
I did very little. And the students, to my mild surprise, did not need me to. What happened instead was a process I recognised without being able to immediately name it: a willingness to let the difficulty sit in the room rather than forcing it toward resolution, a patience with the tension that seemed to assume the room itself would eventually offer a way through. Small acknowledgements. Questions that didn’t demand answers. A quality of attention that was present without being urgent.
It was several minutes before I placed it. It was the particular Irish management of tension in a room — the communal tolerance for unresolved difficulty that operates in Irish social life as a kind of distributed emotional intelligence, held collectively rather than managed by any individual. I had not taught anyone to do this. I had not named it as a practice. No curriculum framework I have ever read describes it as an outcome. It was formation, arriving in a Tamil Nadu classroom because I had carried it out of Kerry without knowing what I was carrying — and recognising it, after fifteen years of working in contexts where I had no particular reason to expect it, felt like watching a river I grew up beside appear in geography I had never mapped.
You don’t notice what formation has made of you while you’re still inside it. You notice it when the same instinct arrives in a context that had no reason to produce it, and you have to ask yourself where it came from. Read more »
A humble post; Hieronymous Bosch seems appropriate here
The first meditation retreat I ever went to was also the worst one, at least circumstantially. A new meditation center was in the process of being built and in the meantime, we were in a series of concrete boxes with tiny fortress windows, fluorescent lights, and corrugated tin roofs with the nails showing. This fit with the original purpose of meditation (the whole point of meditation is to triumph over circumstances with attitude), though not the modern spiritually materialist one. Reluctant renunciates of luxury, we lay on our thin mattresses in our metal bunks, eight to a room, staring at the nails in the ceiling; we ate on benches outside in the summer tropical island humidity, out of tin bowls with tin chopsticks that we washed ourselves. The meditation hall with its industrial blue foam puzzle mat floor and air conditioning was the nicest environment around, which made meditation more appealing. I avoided going to the separate, mold-grown outhouse whenever possible.
I learned years later that there is a practice in Tibetan Buddhism that specifically trains the disgust response: by eating increasingly stranger and stranger foods to you, and reacting calmly, even neutrally, you rewire this evolutionary reaction. (This is also one of the secrets behind cold showers, which I appreciate theoretically: one’s nervous system is meant to greet the cold ever more gently instead of tensing up, which then applies to other things.) So potentially even a miasmic outhouse can become, through training, if not desirable, at least not actively repulsive. Though ask even a well-trained monk what he would truly prefer and you’d be hard-pressed to find one who wouldn’t want a nice hotel room with accompanying restaurant and hot tub over a shanty and gruel.
Meditators are not supposed to care about these things, but of course we do. We are still mammals after all, as my therapist likes to remind me whenever I feel guilty about wanting love and good food and coziness. Worse: we are mammals with minds! In subsequent meditation retreats, the conditions were better, but the materialism was still there because the mind with its meaning-making was (and me with my bad attitude). Then it became about who got the slightly better bed or room, who brought the extra seasoning cleverly hidden in a miniature vitamins bottle (this really happened, and I really was jealous). Not that I didn’t squirrel in my own illicit snacks amidst austerity: a sleeve of chocolate digestive biscuits that I hid amongst my bathing essentials and ate in the shower stall. Read more »

 My cat died of pancreatic adenocarcinoma a few weeks ago. In March she had an annual check up and was deemed to be in good health for 13, although a bit overweight. We noticed that she was walking a little funny sometimes, so the vet suggested we think about arthritis medication. Then one day in May, just before our appointment to start meds for her suspected arthritis, she went into hiding. A more in-depth vet appointment discovered that her changed gait wasn’t from her joints, but from a huge abdominal mass. It took some tests to find out what it was, then came the dreaded decision-making about what to do about it. Apparently cats can live for months with the condition but often with a very dismal quality of life.
My cat died of pancreatic adenocarcinoma a few weeks ago. In March she had an annual check up and was deemed to be in good health for 13, although a bit overweight. We noticed that she was walking a little funny sometimes, so the vet suggested we think about arthritis medication. Then one day in May, just before our appointment to start meds for her suspected arthritis, she went into hiding. A more in-depth vet appointment discovered that her changed gait wasn’t from her joints, but from a huge abdominal mass. It took some tests to find out what it was, then came the dreaded decision-making about what to do about it. Apparently cats can live for months with the condition but often with a very dismal quality of life.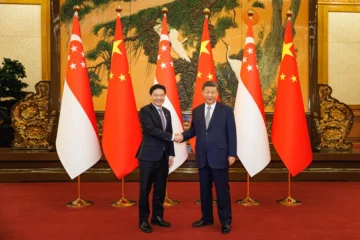




 The Republican Party has forever faced a serious statistical obstacle: There are always more Democrats. Never once since the GOP was founded in 1854 have there been more registered Republicans than Democrats in the United States. Democrats are always more numerous. So how can Republicans win?
The Republican Party has forever faced a serious statistical obstacle: There are always more Democrats. Never once since the GOP was founded in 1854 have there been more registered Republicans than Democrats in the United States. Democrats are always more numerous. So how can Republicans win?
 Dear Readers and Writers,
Dear Readers and Writers,
 About ten years ago, I received an invitation to coffee from a fellow I hadn’t seen in a while. At the time, Rolf Kuhn was teaching English at a middle school in the nearby town of Baden; our acquaintance was the result of our frequenting the same English-language bookstore—
About ten years ago, I received an invitation to coffee from a fellow I hadn’t seen in a while. At the time, Rolf Kuhn was teaching English at a middle school in the nearby town of Baden; our acquaintance was the result of our frequenting the same English-language bookstore—
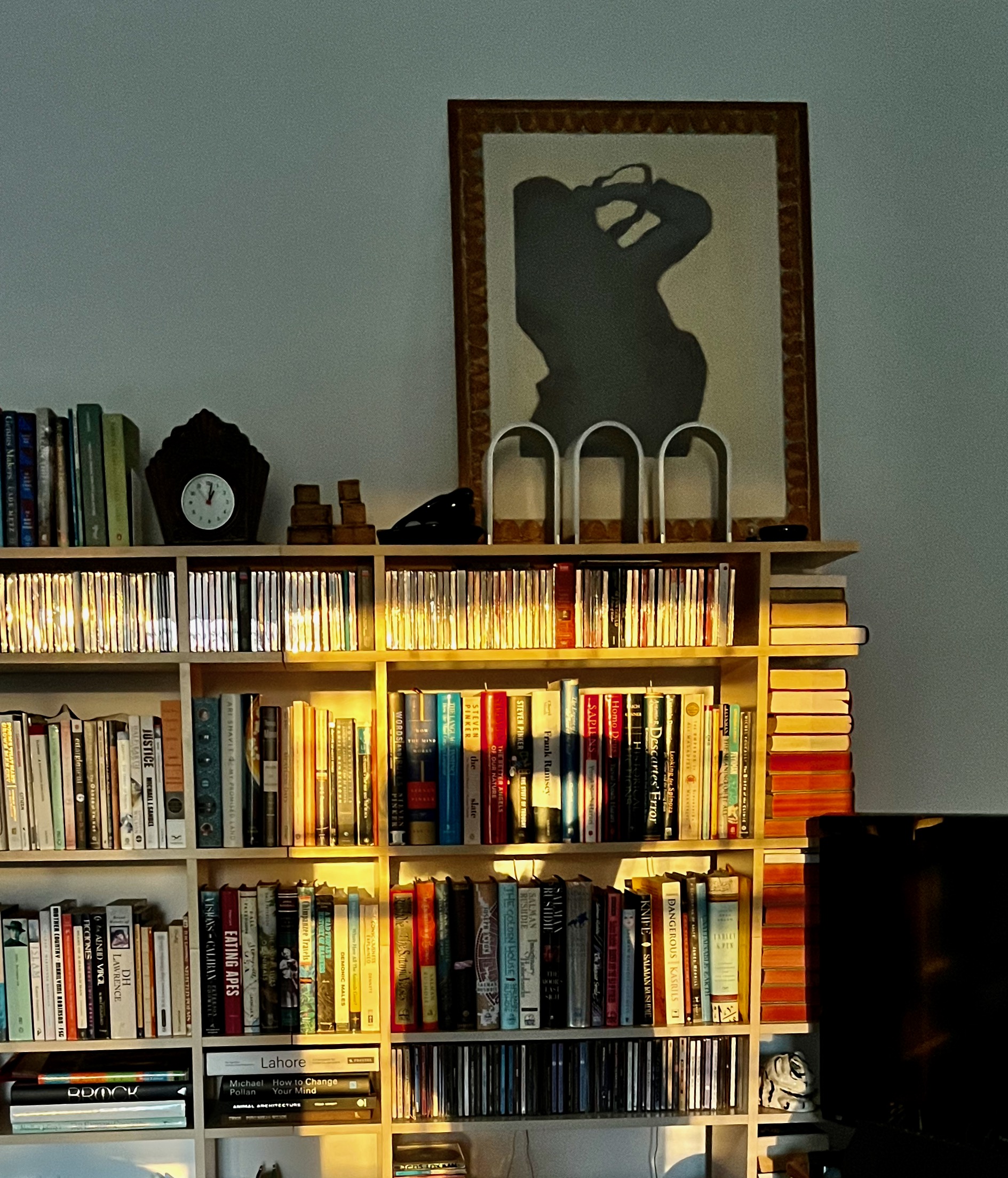 Sughra Raza. Self Portrait In Early Morning Reflected Light. Boston, June 2026.
Sughra Raza. Self Portrait In Early Morning Reflected Light. Boston, June 2026.
 Tycho Brahe was a significant figure in my family. Why? Because my father’s parents were from Denmark, and Tycho Brahe was Danish. Danes were thus important in the Benzon household, as was Danish pastry (wienerbrød, Vienna bread), the real stuff with cardamom seeds, not the fluff you get in diners. And then there is rabarbergrød, a cloudy translucent rhubarb pudding laced with slithers of almonds. Not to mention Danish layer cake, five thin cookie-like layers alternating with custard and currant jelly topped with a lemon-juice & powdered sugar icing, once a year on my father’s birthday. But I digress.
Tycho Brahe was a significant figure in my family. Why? Because my father’s parents were from Denmark, and Tycho Brahe was Danish. Danes were thus important in the Benzon household, as was Danish pastry (wienerbrød, Vienna bread), the real stuff with cardamom seeds, not the fluff you get in diners. And then there is rabarbergrød, a cloudy translucent rhubarb pudding laced with slithers of almonds. Not to mention Danish layer cake, five thin cookie-like layers alternating with custard and currant jelly topped with a lemon-juice & powdered sugar icing, once a year on my father’s birthday. But I digress.