by Marie Snyder
 We want help to know the best approach to take to life. In lieu of church services or complex readings, many turn to influencers for their formulas for “winning” at life that often judge us based on challenging perceptions of beauty or endurance or wealth. The trend towards optimizing provokes people to track everything they do, from the number of steps, to hours of sleep, but for what? To prove they have a right to be here? To belong? To be loved? It definitely doesn’t appear to be making people happier. That may be the cost of simplification of complex advice that edits down more complex ideas into a more superficial draft. The profits come with the reality that it works. People will click on these videos, subscribe to podcasts, and buy all the books. At some point we stopped looking for how to be a good person and instead aimed to be impressive or even just base-line likeable.
We want help to know the best approach to take to life. In lieu of church services or complex readings, many turn to influencers for their formulas for “winning” at life that often judge us based on challenging perceptions of beauty or endurance or wealth. The trend towards optimizing provokes people to track everything they do, from the number of steps, to hours of sleep, but for what? To prove they have a right to be here? To belong? To be loved? It definitely doesn’t appear to be making people happier. That may be the cost of simplification of complex advice that edits down more complex ideas into a more superficial draft. The profits come with the reality that it works. People will click on these videos, subscribe to podcasts, and buy all the books. At some point we stopped looking for how to be a good person and instead aimed to be impressive or even just base-line likeable.
There’s a capitalist benefit to convincing people they’re somehow defective by providing unattainable standards to work towards that, of course, involve products to buy. But it also feels like, culturally, we’re not growing up. Kant called it immature, lazy cowardice whenever people try to figure out how to live by blindly following advice instead of heeding their own reason:
“If I have a book to have my understanding in place of me, a spiritual adviser to have a conscience for me, a doctor to judge my diet for me, and so on, I need not make any efforts at all. I need not think, so long as I can pay; others will soon enough take the tiresome job over for me.”
In the 250 years since he wrote that, we’ve figured out some of the mechanisms that enable us to develop a conscience. We have mirror neurons that help us feel bad when we’ve exploited someone or made them suffer in any way, provided we direct any attention towards them. It’s only possible to be happy while knowingly harming others by not looking too closely at the effect of our actions. Luckily, we’re surrounded by distractions. Read more »
 Imagine this: It is around the mid-1980s and the venerable Sir Georg Solti takes the podium at Chicago’s Orchestra Hall to conduct Rachmaninoff’s Piano Concerto No. 2. The orchestra is poised, the audience breathless.
Imagine this: It is around the mid-1980s and the venerable Sir Georg Solti takes the podium at Chicago’s Orchestra Hall to conduct Rachmaninoff’s Piano Concerto No. 2. The orchestra is poised, the audience breathless. Sughra Raza. Catching Rays. Boston, June 2026.
Sughra Raza. Catching Rays. Boston, June 2026.


 In
In 
 Looking back I see that my undergraduate education—as seen through my three (one merely attempted) majors—was a tour through the grammatical persons. I started out majoring in political science (and studying Latin, to my lasting regret), because I thought I wanted to be a lawyer. Third-person plural.
Looking back I see that my undergraduate education—as seen through my three (one merely attempted) majors—was a tour through the grammatical persons. I started out majoring in political science (and studying Latin, to my lasting regret), because I thought I wanted to be a lawyer. Third-person plural. Road trips were a staple of my childhood.
Road trips were a staple of my childhood.
 Most politicians pledge to
Most politicians pledge to 
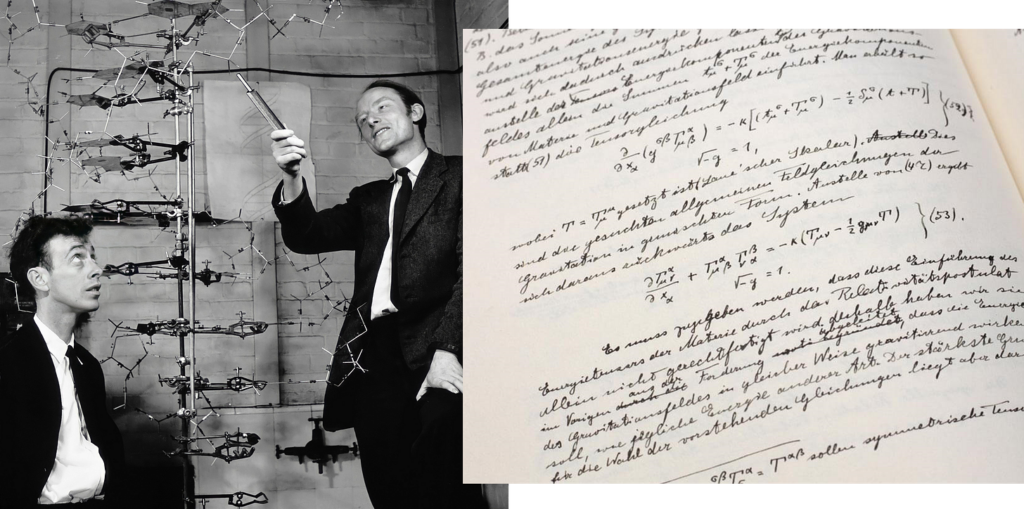 AI is collapsing barriers in scientific disciplines, most notably in math. An 87-year old conjecture named the
AI is collapsing barriers in scientific disciplines, most notably in math. An 87-year old conjecture named the 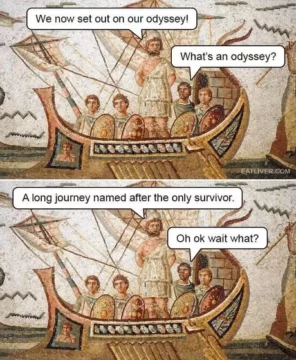 1. The Odyssey
1. The Odyssey Sughra Raza. Fly Paper (sunset series). Late July, 2026.
Sughra Raza. Fly Paper (sunset series). Late July, 2026.